By Michael Gwarisa
In October 2025, Zimbabwe’s National Assembly approved far-reaching amendments to the Termination of Pregnancy Act [Chapter 15:10] of 1977. The proposed changes, introduced through the Medical Services Amendment Bill, 2025, now await consideration by the Senate before possible presidential assent. The outcome will determine whether Zimbabwe aligns its reproductive health laws with its 2013 Constitution, prevailing medical evidence, and contemporary public health realities.
The Senate has emerged as the most decisive constituency in this legislative process. Its approval or rejection will shape not only the legal future of abortion care in Zimbabwe but also the health outcomes of thousands of women and girls who continue to navigate pregnancy under restrictive conditions.
Why the Current Law Is No Longer Fit for Purpose
Zimbabwe’s Termination of Pregnancy Act was enacted nearly five decades ago, at a time when medical technology, constitutional safeguards, and public health data were markedly different. Under the existing law, abortion is permitted only in narrowly defined circumstances. These include cases where pregnancy endangers a woman’s life or health, involves severe fetal abnormalities, or results from unlawful intercourse such as rape or incest.
While these provisions appear protective on paper, in practice they have created high procedural barriers. Requirements such as magistrate approval, certification by multiple doctors, and narrow legal interpretations have delayed care and, in many cases, made lawful termination inaccessible.
The courts have acknowledged these limitations. In 2024 and 2025, the High Court expanded the interpretation of “unlawful intercourse” to include marital rape and sexual abuse of minors, but stressed that lasting reform must come from Parliament. The current amendments seek to close this legislative gap.
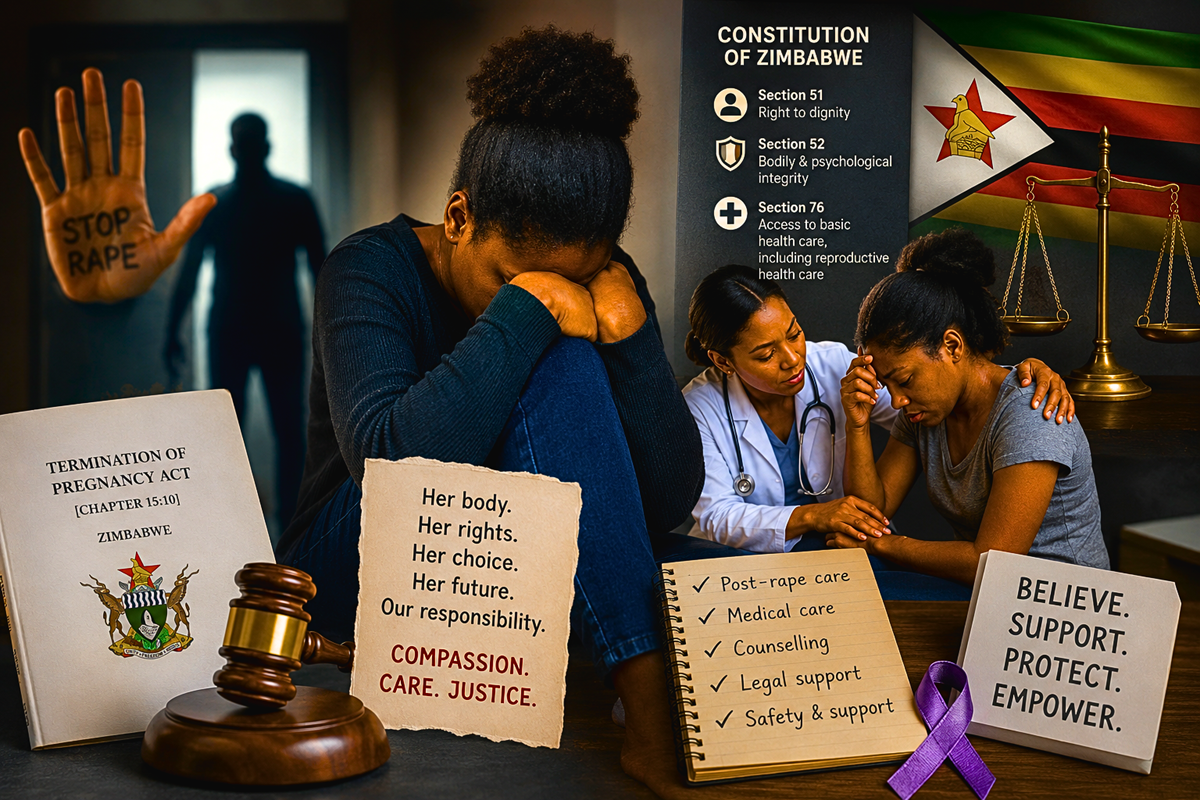
In Mudzuru & Tsopodzi v Minister of Justice and Others and subsequent High Court interpretations in 2024 and 2025, the courts affirmed that constitutional rights to dignity, bodily integrity, and access to healthcare must inform reproductive health law. Specifically, Section 76 of the Constitution guarantees access to reproductive healthcare, while Section 52 protects bodily integrity, placing a positive obligation on the state to remove unreasonable barriers to lawful medical services
What the Medical Services Amendment Bill Proposes
The proposed amendments represent a shift from a punitive framework toward a regulated health services model. Key provisions include allowing termination on request up to 12 weeks of gestation and extending access up to 20 weeks where pregnancy poses risks to physical health, mental well-being, or socio-economic stability.
The bill also removes the requirement for magistrate approval, recognising that abortion is a medical service rather than a judicial process. It proposes expanding the cadre of providers by allowing trained nurses and midwives to offer first-trimester services, consistent with World Health Organization guidelines. Additionally, it permits minors under 18 to consent independently, reflecting constitutional rights to bodily autonomy and access to healthcare.
These changes are not radical by regional or global standards. Similar frameworks exist in South Africa, Mozambique, and Ethiopia, where liberalisation has been associated with sharp declines in maternal deaths linked to unsafe abortion.
The Public Health Case for Reform
Unsafe abortion remains a significant contributor to maternal morbidity and mortality in Zimbabwe. According to the Ministry of Health and Child Care and the World Health Organization, complications from unsafe abortion account for a substantial proportion of emergency obstetric admissions, including sepsis, haemorrhage, uterine perforation, and long-term infertility.
According to the Ministry of Health and Child Care and World Health Organization estimates, unsafe abortion contributes between 6 and 10 percent of maternal deaths in Zimbabwe, with thousands of women treated annually for complications such as sepsis, haemorrhage, and uterine injury. Adolescents and low-income women account for a disproportionate share of these cases, reflecting unequal access to lawful and timely reproductive health services.
These complications disproportionately affect adolescents, rural women, and those living in poverty. Restrictive laws do not eliminate abortion. They simply shift it into unsafe spaces, often involving unregulated providers or harmful methods.
From a public health perspective, expanding access to safe, regulated abortion care reduces hospital admissions, lowers healthcare costs, and saves lives. Evidence from countries that have liberalised their laws consistently shows a decline in abortion-related deaths without an increase in abortion rates overall.
Why the Senate Matters More Than Ever
The Senate plays a unique constitutional role as a house of review, continuity, and moral persuasion. Unlike the National Assembly, it includes traditional leaders, seasoned policymakers, and representatives expected to reflect long-term national interests.
Opposition from some senators, including Senator David Coltart, as well as faith-based actors such as the Catholic Bishops Conference and the Zimbabwe Council of Churches, has framed the debate largely in moral and religious terms. Their concerns reflect deeply held beliefs that deserve respect and engagement, not dismissal.
However, Senate resistance has less to do with legislative mechanics and more to do with values, trust, and perceived societal consequences. This makes the Senate not just a voting bloc but a constituency that must be persuaded through dialogue, evidence, and reassurance.
Addressing Religious and Ethical Concerns Through Public Health Framing
A successful advocacy strategy must acknowledge moral concerns while clarifying what the bill does and does not do. The amendments do not compel anyone to seek an abortion, nor do they force healthcare workers to act against conscience. They regulate access for those who already seek care and ensure it is safe, lawful, and medically supervised.
Public health advocacy should emphasise shared values such as preserving life, protecting women from harm, reducing preventable deaths, and strengthening families. The reality that women are already dying or suffering lifelong complications from unsafe procedures is not a theoretical argument but a documented health crisis.
Framing the bill as harm reduction rather than moral endorsement is essential. This approach has been effective in other jurisdictions with strong religious influence.
Building Senate Buy-In Through Evidence and Engagement
To secure Senate approval, advocacy efforts must move beyond protests and public statements. Structured engagement is critical. This includes private briefings with senators using Zimbabwe-specific data, testimonies from obstetricians and midwives, and evidence from comparable African countries.
Traditional leaders in the Senate should be engaged through culturally sensitive discussions that link maternal health to community stability. Faith leaders can be invited into technical dialogues with medical experts to separate theological doctrine from public health outcomes.
Importantly, advocates should emphasise constitutional obligations. Section 76 of the Constitution guarantees the right to healthcare services, including reproductive healthcare. Section 52 affirms bodily integrity. The proposed amendments seek to operationalise these rights within a regulated legal framework.
A Path Forward That Balances Law, Health, and Values
The Senate has an opportunity to shape a law that reflects Zimbabwe’s constitutional commitments while safeguarding public health. Rejecting the bill would not preserve the status quo. It would perpetuate a system that quietly transfers risk from law to women’s bodies.
Passing the amendments, with clear safeguards and ongoing dialogue, would acknowledge the reality that reproductive health policy must be grounded in evidence, compassion, and the lived experiences of women and girls.